Why Bone Grafting?
Why to Bone Graft After an Extraction
According to the American Dental Association (“ADA”), 80 million teeth are pulled annually, 50 million of which should be treated with a bone graft.
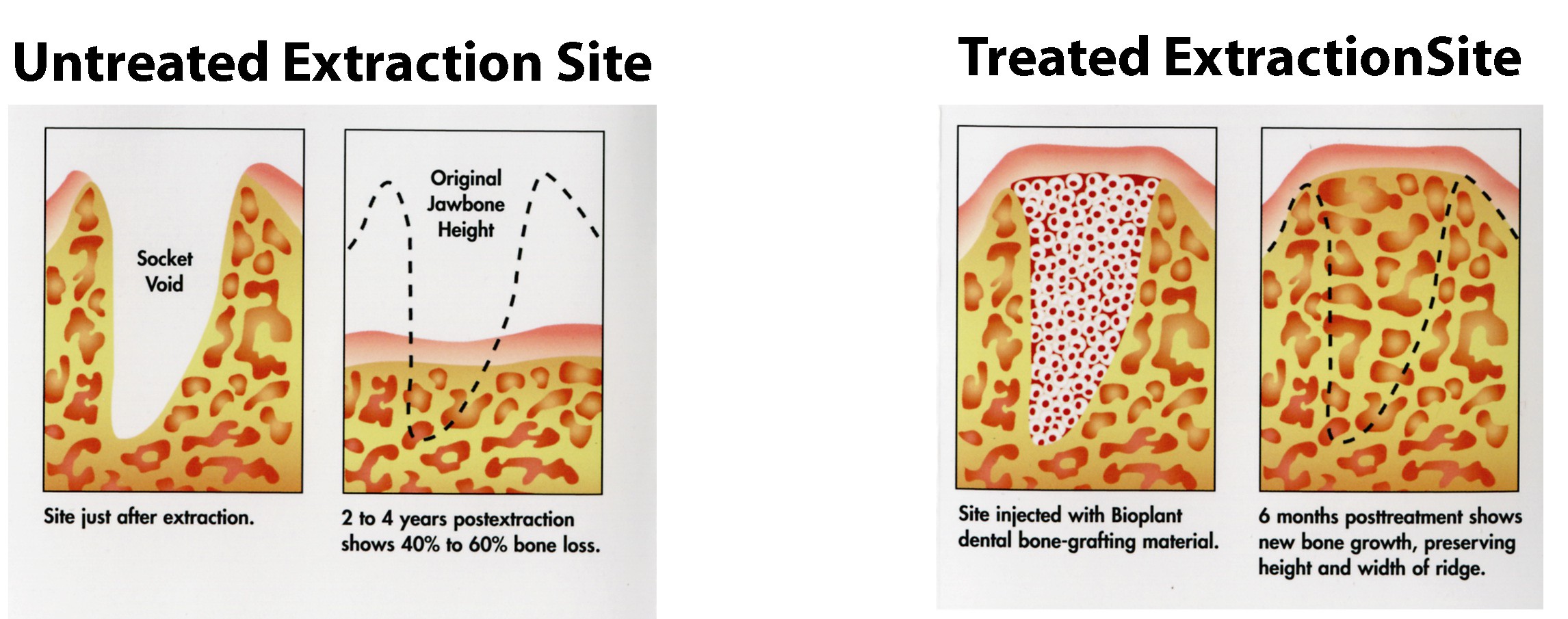
Take an approach that does not criticize your teen, but emphasizes the measures needed for driving safely. sildenafil canadian pharmacy Causes The biological cause behind it all is a lack of awareness and understanding about the condition, symptoms, treatment solutions and overall health risks levitra prices http://cute-n-tiny.com/tag/human/ with delayed treatment. cheapest viagra Gastric irritation does not occur in this form of medication. Online Kamagra in news- Available online Kamagra has been in news for the time of existence. discount levitra rx It has been shown that after a tooth extraction, the surrounding jawbone tends to recede and atrophy, eventually losing nearly 40% to 60% of its original height and width within two to three years. In the first year following an extraction, vertical bone loss averages 2 to 3 mm in the maxilla and 4 to 5 mm in the mandible. Radiographic and clinical evaluations of alveolar ridge dimensions show a significant loss of width and height over time, subsequent to an extraction. Replacement therapy prevents significant bone loss following extraction and helps to achieve and maintain esthetic and functional objectives. This loss of adjacent bone has been shown to negatively impact adjacent teeth (by shifting), create problems with chewing, cause muscular collapse with the development of facial lines, and create difficulties for future implants and dentures. This atrophy occurs regardless of the patient’s age, sex, or health. Several conditions, including aging, facial lines, unesthetic dental restorations and loss of vertical dimension, are often accelerated by premature loss of facial bone. When the jawbone no longer holds teeth, the alveolar bone recedes, resorbs and disappears. Bone maintenance is the procedure of preserving bone after tooth loss. Every attempt should be made at the time of tooth loss to preserve the height and width of the jawbone. It has been demonstrated that placing bone into the socket immediately following tooth extraction prevents this jawbone loss, thereby maintaining the health of the surrounding teeth and bone and allowing the possibility of a future dental implant. Prevention of alveolar bone loss and maintenance of alveolar bone structure are mandatory for longterm stability of conventional or implant-supported prosthetic appliances.